|

|
Overview
Heart failure currently affects 2% of the western population and 10% of people >75 years. In about 50% of patients with heart failure occures with preserved pumping ability of the heart (heart failure with preserved ejection fraction - HFpEF). Once patients develop symptoms, the prognosis is poor.
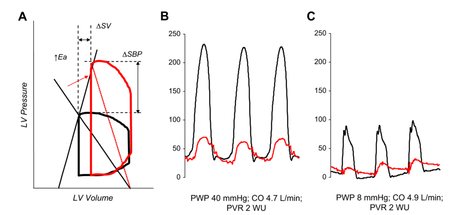
Figure 1. PV Loops measurements in HFpEF. From Borlaug and Kass. Heart Fail Clin 2010
|
HFpEF is one of the major unresolved areas in clinical cardiology. The gold standard diagnosis is made by way of an invasive assessment of haemodynamics using PV loops, requiring expert skill and experience (Figure 1. Borlaug et al 2010). In practice, the diagnosis is more often one of the exclusion, following on numerous investigations to exclude other specific heart diseases. Although, many echocardiographic parameters, including dilated left atrium and raised E/e' are found in HFpEF, these are non-specific and indirect markers often found in other cardiomyopathies (hypertensive, hypertrophic, amyloidosis).
|
|
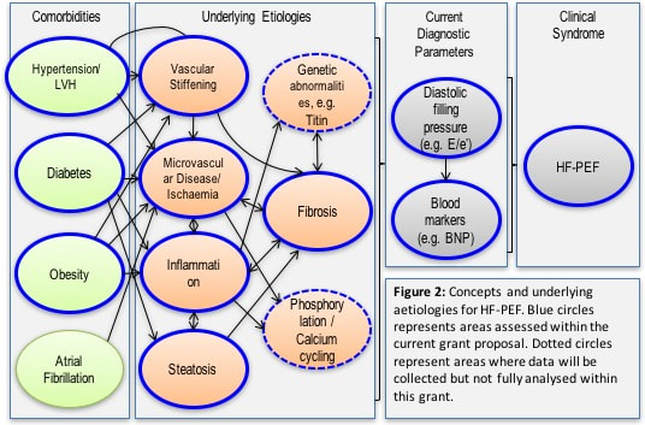
Currently, no noninvasive diagnostic method allows to reach the diagnosis of HFpEF diagnosis. Cardiovascular magnetic resonance (CMR) is an excellent diagnostic tool, which is routinely used to determine numerous heart conditions which lead to heart failure (such as those mentioned above). In addition to specific diagnoses, many CMR parameters can directly relate to the underlying pathophysiological processes, including myocardial fibrosis, inflammation, infiltration and steatosis. These processes are thought to be commonly associated with HFpEF (Figure 2). To-date, no validation of novel CMR parameters versus the gold standard of invasive haemodynamics in HFpEF has been performed. The underlying histopathological substrates also remain poorly explored. The utility of CMR in supporting insight into the various underlying pathophysiologies leading to HFpEF has not been formally assessed.
|
|
We propose to undertake the first systematic comparison between a comprehensive CMR protocol and invasive haemodynamics as the best possible gold standard, as well as define the histopathological drivers in myocardial biopsies. Additionally, we will examine the relations with tissue and serological biomarkers implicated in HFpEF. We will also examine the role (and agreement) with standard and novel parameters by echocardiography e.g. the change of filling parameters during ergometric stress.
Aims of the StudyWe will examine the relationships between the readouts of novel CMR measures, providing high density, in-depth tissue phenotyping, with the gold standard of invasive haemodynamics in patients fulfilling the diagnosis of HFpEF.
Methods and DesignThis is a multi-centre controlled validation study in a total of 110 patients fulfilling the diagnostic criteria for HFpEF. Additional groups of subjects will be recruited to serve as age-matched controls and assess reproducibility of methods.
The study protocol was reviewed and approved by the Frankfurt Institutional Ethics committee. All study procedures are carried out in accordance with the Declaration of Helsinki (2013). Written informed consent is obtained from all participants. Study registrationwww.clinicaltrials.gov (NCT03251183)
|
Participating sites
FundingThe study is funded by a project grant from the German Centre for Cardiovascular Research (Call for Early clinical studies).

Decipher HFpEF Material is available on DZHK Internal Website
Current statusEnd of Recruitment
|

|
|
